

As communicators, we’ve always known that communications is an essential service to the effective running of an organisation. But not everyone else has always shared that view. Maybe the times they are a changing…
by Amanda Nash
Communications is listed as an essential service in our major incident plan. We have our own departmental major incident plan too. But sometimes it’s hard to believe, I mean deep down believe, that we’re essential, when you compare us to other essential services listed in the plan – like our Emergency Department (A&E).
Working in a large, specialist hospital and Major Trauma Centre in Plymouth, it’s important to understand Communications is one of many important support services and our role, our raison d’etre, is to be there to support the care of patients. That’s exactly as it should be.
But sometimes the doubt about how important our role is creeps in. Imposter syndrome in a strange cloak. As I stood in my son’s playground on the last day before schools closed, I had a moment of doubt – are we really critical? What would happen if my son had to take a school place meant for real key workers, i.e. those in uniforms?
But pausing to look back on the first month, no six weeks of COVID19, have reminded me that Communications is indeed an essential service. From the moment I first accompanied clinical colleagues walking round our hospital to scope out which ward would be the starting ‘red zone’ for our Covid-positive patients, to mid-April when a number of wards in our hospital are designated for patients who have tested positive, we haven’t stopped.
Our Communications Team has been flat out and our strategic focus has been two-fold:
Communicating with staff
Communicating with patients and relatives
We started our first daily staff bulletin on 3 March. Communications theory and neuroscience tell us that during a crisis, when a major threat is perceived, clear communications with a regular drumbeat is critical. The pull from staff for information has been great and grown greater day-by-day.
As a Communications Team, we were already used to sharing a daily email with all staff. But the COVID-bulletin as it quickly became known, overtook that as the must-read. To date, the bulletin has included everything from clinical algorithms and updated infection control policy to messages for staff about everything from free car parking to individual examples of #CovidKindnessUHP. Our staff are great at showing initiative and kindness to patients and each other. We don’t have to look far.
Let me be clear – these daily bulletins aren’t simply broadcasting. We use the soft and hard intelligence we get back from staff to drive what information we share. What do staff want to know about? What are the current and emerging issues? We make a point of rooting out questions and issues, for example, myself or one of the team accompanies a Deputy Medical Director to talk with the junior doctors several times per week. We try to make a point of asking colleagues what they want and need and then to close that circle.
We have had fantastic feedback from colleagues throughout our 7,000+ strong #1BigTeam on what we’re doing. Colleagues have told us in corridors, popped their heads round the door (at a safe distance) and even written to us to say things like:
“I have been impressed with the comms that you are doing currently. Keep it up!”
But, little did I know on 3 March, this was the start of what will probably be turn out to be a long and quite hard marathon. So far as a Communications Team we have:
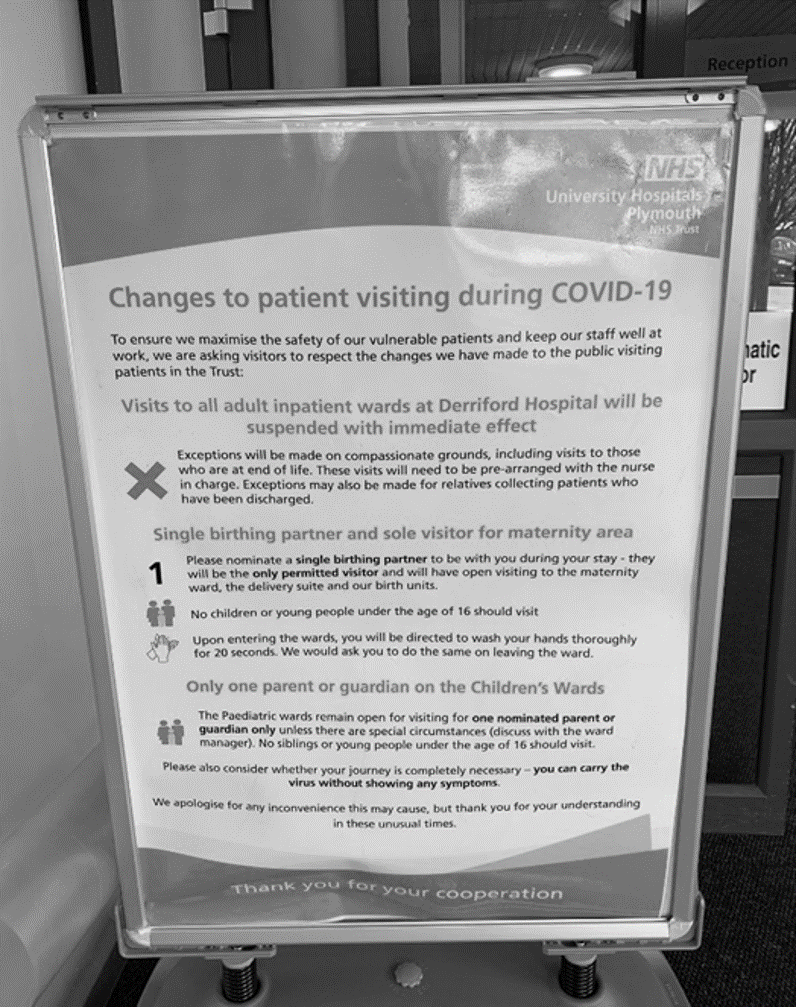
Communicated changes to visiting hours three times. We have gone from open visiting to virtually none at all. We have designed, made and erected large signs, shared on social media and communicated internally.
Attended daily meetings to understand and input into our organisation’s planning and response to COVID-19. We have a fantastic Chief Exec and Exec team who understand the value of good communications.
Liaised with our Infection Control Team and made videos about how to safely put on and take off Personal Protective Equipment (PPE); how to take a swab and with our military colleagues, we have undertaken work on psychological preparedness. We have linked with Occupational Health, our counsellors and psychologists.
Enabled three virtual meetings of our 300+ consultants, helped them be interactive with the use of Slido questions and advised them on possible topics and key themes to address.
Filmed two videos with our Chief Executive intended primarily for our #1BigTeam of staff but also made these public recognising how much interest and support there has been from our local community. The first is HERE.
These videos have led to coverage from our local media, who have been extremely supportive, for example Plymouth Live here and ITV Westcountry here
Filmed 40+ sessions with colleagues in Training and Development to enable all the new staff joining our organisation to have a virtual induction. This is key as we have been recruiting hard, for example for additional domestic staff.
Worked with our wonderful colleagues in HR and Organisational Development to create a Support Hub for staff and Advice and Guidance hub and we’re hoping to work together with our clinical leads to run a virtual Schwartz round in the coming weeks, if we can.
Advised colleagues on the impact of changes to clinical services, communicated changes to patient appointments and written and advised on patient letters and other forms of communications.
Supported a switch to virtual outpatient appointments – Attend Anywhere – and our Communications Team member has been a critical part of the project team. She is regularly praised and thanked by the project lead for her hard work on helping get this up and running.
Worked with colleagues to share stories of staff returning to clinical duties of secret garden retreats for staff to unwind in and of patients who have been cared for with COVID-19 leaving hospital
Created signage for Red and Amber zones and COVID-19 notice staff boards with poster pockets in them for every ward and department so staff can include the daily bulletin and policy documents in them. These can then support staff briefings.
Supported colleagues in doing media interviews, used social media relentlessly and our website has come back into force as a repository for information, for example around all the changes to services we are making.
We have listened, advised and liaised with so many wonderful colleagues inside and outside of our organisation ... it hasn’t always been plain sailing by a long chalk. When you’re having to take big decisions quickly under pressure, it’s hard and I learned in the early days, it’s not enough to be kind. We have to be even kinder, to others and to ourselves.
If the above are examples of ‘What went well’, I think it would have been ‘Even Better If’ we had had time to do some more work with the media. But our whole team, split into half working at home and half in the hospital, to support physical distancing and limit the risk of us all being affected at once, simply hasn’t had time, despite starting early, finishing late and working weekends and Bank Holidays.
We’ve also started evaluating – we know, for example, that a single post about a patient leaving hospital and the number of discharges we have had, reached more than 124,000 people with an engagement rate of 12.5k on Facebook alone. But I have to confess our bigger evaluation document is only partially structured and keeps slipping to the right of our agile board as one ‘to get to’.
What is most rewarding though, is two things that have helped patients and their families. The pain of patients on our wards not being able to see their families and loved ones is almost tangible. Being separated from your family when you are unwell is hard, add into that living through a time of great uncertainty and anxiety, and it must feel immensely tough. I know our frontline staff feel this acutely and they talked to us about this.
Several weeks ago, a colleague in Patient Services came to me with an idea – why not use the iPads we normally hold for patient satisfaction surveys for patient and family communication?
So began a #TeamEffort with our amazing colleagues in Patient Services and IT: we wheeled and dealed, found as many iPads as we could get our hands on, set them up so Zoom could be loaded onto them, wrote instructions for ward staff and got them onto wards so staff can help patients video-call with their families. Our first trial took place with a patient in Cardiac Intensive Care late one Friday night. It worked. We then started work on wider rollout.
Feedback is starting to come in – this weekend one family told us on social media:
Our family did this yesterday, first time we had seen our Dad in 4 weeks! The hospital have been amazing
We’re still scouring the hospital for any spare iPads, because as one Palliative Care Consultant told us, we don’t need one per ward, we need two!

We have also set up a scheme called Send your loved one a message One of our doctors from Health Care of the Elderly (HCE) messaged me late one Friday night to see what we could do:
Hello! I appreciate you have a huge amount on... but please can I make a request from our HCE wards? We have a lot of very poorly patients in who have nobody to visit and their families can’t get out to send them cards. Any chance of an appeal to ask the public to send us some get well soon cards for our lonely older people please?!
I knew we could do better than that! In another #TeamEffort with Patient Services, we created an online form that families fill in with their message and send us a photo if they like. We print out the messages and photo, include them in a ‘Thinking of you’ card and deliver them to wards and ICU areas (including over Bank Holiday weekends). I know we’re not the first hospital Trust to do this but the difference it is making can’t be under-estimated.
One nurse commented:
I received one of these this week for my patient and he was thrilled to have it read to him- both of us were very emotional. Fantastic idea xxx
As I write this, what I reflect on most is the fact that Communications is a small but essential part of #1BigTeam. And there are many more essential teams like us – working in Estates and Facilities, HR, labs, clinical engineering and many more.
Every day we work with some incredibly skilled and compassionate colleagues, clinical and non-clinical, who all have the interests of patients at heart.
I didn’t need my son’s key worker place at school as my husband can work from home.
But as I reflect back on these first weeks and think ahead to what is to come, I know how hard colleagues in communications teams up and down the country are working. And I am convinced that communications professionals supporting NHS and other essential local government services should be proud to call themselves key workers.
Amanda Nash is head of communications at Plymouth Hospitals NHS Trust. You can say hello on Twitter at @manickmanda
*Sign up for the comms2point0 eMag*
The comms2point0 eMag features exclusive new content, free give-aways, special offers, first dibs on new events and much, much more.
Sound good? Join 2k other comms people who have subscribed. You can sign up to it right here.
